This first part written in late Feb, 2016 and concerns the first OAT test I did in mid-2015, plus more.
Then in red, you’ll see an Update for September 2016 after I had a MAJOR crash, plus did a second OAT right smack in the middle of that crash.
Then comes another Update in red for 2017 where I discovered I’ve had mold in my body all this time…perhaps the bottom line for ALL of this.
FEBRUARY 2016: I am a hypothyroid patient who discovered in a hard way that there can be more issues going on that need to be addressed, apart from one’s hypothyroid state!
And the Organic Acids Test might be key to understand what is going on.
Sure, treating our hypothyroid state in a correct way is huge for health, energy and well-being, since thyroid hormones effect virtually every cell and organ in one’s body! In 2002, I went from 20 years of “hypothyroid treatment hell” with T4-only meds like Synthroid and Levoxyl, to turning my life around in a HUGE way by changing to Natural Desiccated Thyroid and finding my optimal dose, as well as optimizing issues related to years of a former bad treatment.
But due to a few back-to-back incidents over the past year, it dawned on me that something else is going on with me. For example, I found out, when detoxing high copper levels in 2015 for six months (my fault–not due to MTHFR–another story) that something is clearly wrong. I had horrific and debilitating fatigue the entire time I was detoxing–far worse fatigue than I’d seen others have. It made no sense to me.
So because of this debilitating fatigue, I decided to learn more about myself and ordered an Organic Acids Test (OAT) in the summer of 2015 while detoxing high copper, which is done via testing your urine. Now it’s somewhat expensive–it can start at $345 and up from there. But what it can reveal about you is huge. I discovered, among other issues, that I definitely have a mitochondrial problem, plus other issues that are probably inherited—carb metabolism problem and fatty acid issue. I started on their recommended supplements.
But in February 2016 as I am writing this, I went back to those results. I had a horrific crash after a day of activity which left me in bed awhile, and took weeks to recover from. This was after lowering high copper, treating SIBO (due to the high copper) and was actively treating a yeast infection from hell. My iron was also good. So what was that horrific crash and unrelenting fatigue about??
WHAT ARE ORGANIC ACIDS?
The Organics Acid Test (OAT) examines metabolites (chemical substances produced by your metabolism) that are coming out in your urine. Those metabolites can give clues about the efficiency (or lack of) of your internal cellular processes as well as gut microbes. It gives clues if we have a blockage, nutritional insufficiencies, and/or bacterial overgrowth.
Organic acids are the byproducts of cellular metabolism, i.e. your cellular metabolism is made up of certain steps of certain biochemical reactions and pathways based on your body’s needs. So if my body needs energy, for example, certain metabolic reactions occur down a pathway to create that energy. Like this: A to B to C to D. Or if I need to break down the food I eat, there are certain metabolic chemical reactions needed. And in creating those different metabolic pathways, certain acids are used and/or produced. They range from acetic acid, butyric acid, oxalic acid, lactic acid, malic acid, uric acid, citric acid and more. https://en.wikipedia.org/wiki/Organic_acid
But sometimes, those metabolic pathways don’t work the way they should! So A might break down to B, but it stops there and begins a different pathway. Because of a nutrient deficiency or an inherited block, they go down DIFFERENT pathways in trying to create the same end result, but which can be inefficient or problematic. And what comes out in your urine reveals what can be going on inside you that’s inefficient or needs help.
WHAT THE ORGANIC ACIDS TEST REVEALS
The results tested are basically listed like this (for the ORGANIC OAT test by ORGANIX, which is the first one I did):
1. NUTRIENT MARKERS, which reveals what is going on with your Fatty Acid Metabolism, your Carbohydrate Metabolism, and your Energy Production (aka Citric Acid Cycle, also called the Krebs Cycle). You also learn if you have enough of certain B-Vitamins, and how they are affecting (or not effecting) your Methylation abilities, plus other nutrient deficiencies. There’s potentially a lot of information under all of this.
2. CELL REGULATION MARKERS, which is looking at your Neurotransmitters, plus Oxidative Damage and Antioxidants.
3. TOXICANTS And DETOXIFICATION indicators i.e. what toxic element might be to high in your body, plus whether you are detoxing (which I was).
4. BACTERIA OR YEAST MARKERS
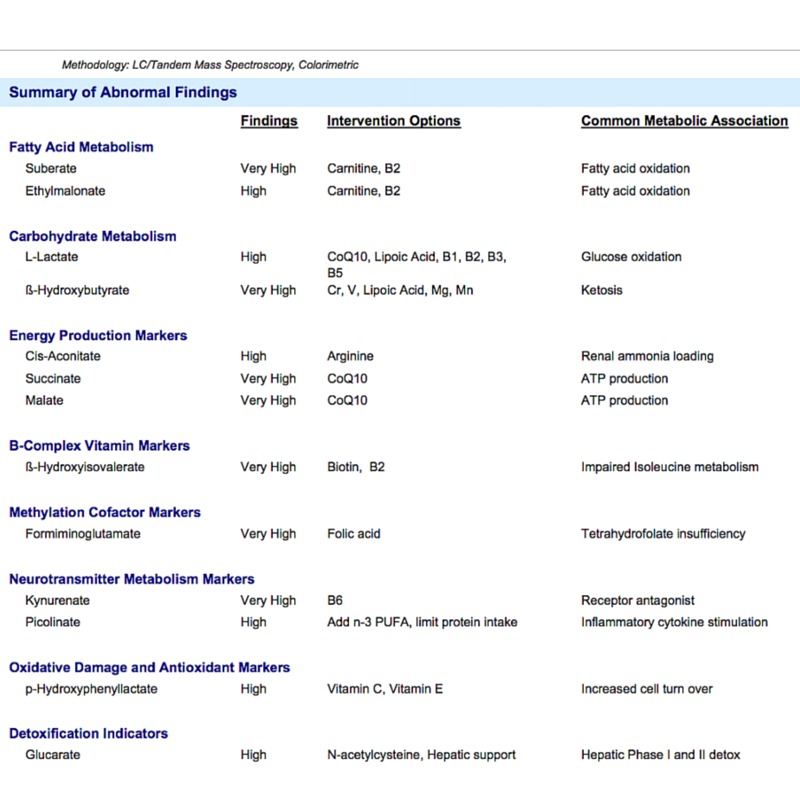
HOW MY OAT RESULTS LOOKED IN JULY 2015–my first OAT testing
Below you will see what abnormalities based on what was coming out with my urine, what they recommended I do about those problems, and what those problems are commonly associated with. Note that there were other areas tested that are not shown below because they were fine….though I do mention two of those under the Energy Metabolism area that were so close to high!!
THE MEANING
Interpretation of all the above has NOT been easy. First, I could find NO doctor anywhere in my area who either understood this, or even accepted it. When I told one PA what I had discovered about myself in one particular result, he proceeded to pooh-pooh the entire Organic Acids Test without even asking how my symptoms match the implications. All I could think of is “Are practitioners really this stupid, close-minded and clueless” as I walked out. (They are).
So I had to begin extensive research on my own on the internet. And it’s not easy. First, there are YouTube videos that helped a lot at the beginning and I highly recommend them. This is one: https://www.youtube.com/watch?v=x92N2wgM0J4 You are faced with understanding biological and medical terminology that can be daunting. But those videos do help!! Search for others. And my article here will help you as a start.
Then I started doing research on the net, just with certain terms. For example, I would search the word of whatever compound I was quite high in, such as “high urine Cis-Aconitate”. And there is plenty to read, and again, I frequently had to read certain articles or certain parts of articles several times to really get it to soak in. I can’t stress the latter more–read, read! But then came weeding through it all and deciding “what information applies to me?”. Because some of the information was pertaining to blood, not urine, or certain diseases that involved the particular compound vs other causes. (I also learned to always add “high urine “to each my search word results)
I also had to deal with a tendency of mine to be overwhelmed or bored. I simply had to come back to it another time.
Then when it came to recommended nutrients to treat some of these issues, there was the problem of “how much” of each do I take. The OAT results had recommendations, but I found some of it to be quite paltry and/or ineffective, and I’ll talk about that later.
DID I SEE A CLUE AS TO WHY I WAS SO DEEPLY TIRED WHEN DETOXING HIGH COPPER? YUP.
Yes! One of the first things that stood out to me in my OAT results was under Energy Production (Citric Acid Cycle). I clearly had a big problem there, and I think the high copper, then the detoxing, either caused it or made what I had much worse!!
The Citric Acid Cycle (also called the Krebs Cycle because of the man who identified it) is the way your body generates its energy via a series of important chemical reactions. It’s all derived from the carbohydrates, fats and proteins that you consume. https://en.wikipedia.org/wiki/Citric_acid_cycle
In my urine results, there were three particular substances which were quite high in my urine and shouldn’t have been if things were working the way they were intended: Cis-Aconitate, Succinate and Malate. And what you don’t see in the above, but was on another chart of reference range “graph lines’, was that both Citrate and Hydroxymethylglutarate were nearly high, too—also associated with energy production.
In other words, there are FIVE clues that I have a faulty energy metabolism, i.e. my ATP production (that which supplies large amounts of energy to my cells) was probably less-than-optimal due to a blockage or inhibition and thus, there was a movement towards a “compensatory pathway” to get energy, which these high levels revealed. And frequently, those compensatory pathways are not wonderful ways to achieve good energy. In simple terms, I do not make great energy…
And because each metabolic pathway requires certain enzymes and nutrients to achieve the end result, my OAT information stated that these specific high acid levels imply that I am deficient in two key nutrients: Arginine (high Cis-Aconitate) and CoQ10 (Very High Succinate and Malate), plus several B-vitamins. It turns out that adequate amounts of CoQ10 are critical for the mitochondrial in the formation of the energy-producing ATP!! (And in 2017, I finally figured out that my body was not producing CoQ10 anymore, probably due to the stress of the massive Mold Inhalation I went through in 2013. i.e. the latter may have activated some genes which influence CoQ10 production)
For Arginine, I expertly ignored that at the beginning when I got my OAT results. i.e. overload and boredom. But it was one of those later times of study that it hit me: I REALLY need this stuff. My high Cis-Aconitate can be due to ammonia toxicity (either via a slow renal process or the high bacteria I found myself with) and that ammonia toxicity can indicate arginine insufficiency, since arginine is needed to achieve the ammonia clearance through the Urea Cycle. Says one study: The high concentration of ammonia interferes with oxidative metabolism in the brain through an inhibitory effect on the tricarboxylic acid cycle (TCA). Inhibition of the TCA cycle may result in depletion of ATP. https://www.ncbi.nlm.nih.gov/pubmed/9475502 My high ammonia depletes my ATP, which depletes my energy!!
Arginine is one of several necessary amino acids and is used in the biosynthesis of proteins i.e. a “multi-step, enzyme-catalyzed process where substrates are converted into more complex products”. And this points to another problem I found out I had via the OAT–I don’t break down proteins in the right way, and it recommends I eat much lower amounts of protein. Perhaps this is due to my low arginine?
Additionally, my Citrate (shown on the line graph you are not seeing) is almost high which also goes along with arginine insufficiency. Remember the name of this energy process–the Citric Acid Cycle?? So you can see that Citrate is important, yet mine is coming out in my urine instead of being used properly. Isocitrate was heading up on the line graph, as well–also a sign of arginine insufficiency. All also related to Krebs Cycle i.e my energy metabolism.
But another problem ensued: HOW MUCH arginine?? I did a lot of research again…it’s maddening. But did see some are on 2000 mg, 5000 mg or 10,000. I am on 1000 as I am writing this, but I also take 500 mg of Ornithine with it, a precursor. Ornithine, along with Arginine and Citrulline, are the three amino acids involved in the Urea cycle, alongside L-Arginine and L-Citrulline. Here’s a study with showed the Ornithine improves energy, which seems to be because it lowers ammonia: https://www.ncbi.nlm.nih.gov/pubmed/19083482
I discovered that Citrulline (the precursor of arginine) efficiently increases plasma arginine concentration in healthy adults without any reported side effects that high dose arginine could have to your stomach https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3268370/
I also found out that Ceylon type Cinnamon metabolizes into sodium benzoate, which chelates ammonia (which again, I’m assuming is high due to low arginine–no testing done yet). When I remember, I do 1g-2g in the evening, mixing it with either yogurt or cream cheese. 1 tsp of ground cinnamon is 2.6g. If anyone uses a capsule machine one “00” capsule would be about 1/2g. More great info here: https://raypeatforum.com/community/threads/too-much-protein-at-once.5455/
An interesting tidbit about low arginine: it may be linked to Alzheimer’s: http://www.nutraingredients.com/Research/Arginine-deficiency-may-be-linked-to-Alzheimer-s And it says that arginine supplementation can’t get through the blood-brain barrier, so the solution is to block arginase which breaks down arginine!! L-norvaline blocks arginase. But I’m to ask my doctor to find an arginase test for me.
The bottom line is: I have strong evidence of poorly functioning energy production….and the energy it probably took to detox was greater than I had the ability to keep up with…thus my constant deep fatigue. As of Feb, 2016, I am currently taking 500 mg CoQ10 (I had to go higher. See my September 2016 update below), 1000 mg Arginine and 500 mg Ornithine, arginine in another supplement, plus the Ceylon cinnamon to see if I notice improvement.
And by the way, articles say that Creatine stimulates the ATP, so I have just started that today. (Didn’t keep up with it)
A SIDE NOTE CONCERNING THE TERM “CHRONIC FATIGUE SYNDROME” aka CFS
I have noted that Dr. Myhill believes that the term CFS fits what is actually a mitochondrial problem — similar problem to my “energy metabolism disorder”. And she uses the CFS label throughout her great information.
But I am totally turned off by the term CFS. I remember the 1980s when it was heavily coined as this “new” and “mysterious” condition that also included reactivated EBV for many. Later, thyroid patients were getting the CFS diagnosis a lot, too. But they discovered that once they got on Natural Desiccated Thyroid AND found their optimal dose, that “chronic fatigue” went away. For most thyroid patients, CFS aka chronic fatigue was NEVER a “separate” condition as doctors have so often pushed because of their inane need to use the TSH lab test (which leaves many undiagnosed hypothyroid and thus, fatigue) or Synthroid when they do treat (which is lousy being only one of five thyroid hormones, and thus continued fatigue.). See https://stopthethyroidmadness.com/t4-only-meds-dont-work
Then you have so many die-hards who think that “CFS” equals “EBV”. Black and white. One and the same. But our experiences have not found that to be true. Sure, you have chronic fatigue with EBV. But some have chronic fatigue without it.
Instead, I see myself as having a “Mitochondrial problem” which does not include reactivated EBV, is not “mysterious”, and is not poorly treated hypothyroid since everything for me is perfectly treated in that arena. I also have optimal iron levels as just tested, and I do not have adrenal fatigue. It appears that many who are assigned the CFS/ME moniker have either undiagnosed or poorly treated hypo, inadequate levels of iron (versus optimal) and a cortisol problem (which only saliva should be used to discern, not blood.
And in spite of her use of “CFS”, she has a good page about the mito problem: http://drmyhill.co.uk/wiki/CFS_-_The_Central_Cause:_Mitochondrial_Failure
I ALSO HAVE A CARBOHYDRATE METABOLISM DISORDER
It’s stated that a carbohydrate metabolism disorder is a “congenital abnormality” i.e. inherited. https://en.wikipedia.org/wiki/Inborn_error_of_metabolism And oh did that make sense, as my Dad’s side of the family ALL had diabetes (but only if they got fat). Luckily I don’t have it, but clearly, this could lead to it. Lovely.
What revealed this issue is my high L-Lactate and very high B-Hydroxybutyrate. For the “excess L-Lactate” http://emedicine.medscape.com/article/167027-overview states that it represents increased anaerobic metabolism due to tissue hypoperfusion. Anaerobic means lacking in oxygen, and hypoperfusion means an inadequate supply of oxygen and nutrients to the tissue. And this is where my faulty Citric Acid/Krebs Cycle again rears its ugly head.
Here’s what http://emedicine.medscape.com/article/167027-overview states is supposed to happen:
The anaerobic metabolic pathway known as glycolysis is the first step of glucose metabolism and occurs in the cytoplasm of virtually all cells. The end product of this pathway is pyruvate, which can then diffuse into the mitochondria and be metabolized to carbon dioxide by another, more energy-efficient metabolic pathway, the Krebs cycle. The metabolism of glucose to pyruvate also results in the chemical reduction of the enzyme cofactor oxidized form nicotinic acid dehydrogenase (NAD+) to nicotinic acid dehydrogenase (NADH) (reduced form).
The same above article states:
Lactic acidosis (I always seem to have a lot of that), on the other hand, is associated with major metabolic dysregulation, tissue hypoperfusion, the effects of certain drugs or toxins, and congenital abnormalities in carbohydrate metabolism.
And if my Krebs cycle is faulty, which my results show it clearly is, I tend to make too much l-lactate for energy, and it doesn’t get used well!! Lovely. My Carbohydrate Metabolism Disorder contributes to my Energy Metabolism Disorder if I’m understanding all this correctly.
My carb disorder also tends to mean that I use muscle for energy instead of fat. That’s why to the right of my very high ß-Hydroxybutyrate, you see “ketosis”. I’m in a chronic state of ketosis, just like my diabetic husband, even tho I’m not diabetic! He also has high ß-Hydroxybutyrate!! Ketosis means I’m not using my carbs for energy but using my fat and making ketones…
I’ve read that high ß-Hydroxybutyrate means you have impaired insulin function, which some call insulin resistance. But it can mean that the insulin issues could impact the transport of amino acids into the cells. And that’s where arginine can be important—it’s stated to improve the sensitivity of the body’s cells towards insulin. http://www.aminoacid-studies.com/areas-of-use/diabetes.html The latter article says the same for l-carnitine in improving sensitivity to insulin. Because I’m on both. If that’s the case, Arginine could ultimately improve my energy cycle”I hope,…since so far, the l-carnitine hasn’t done much that I’m aware of. I’ll talk about it more below under Fatty Acid.
You’ll see that CoQ10 is recommended again for a carb metab disorder, plus ALA and the B-vitamins. But for the high ß-Hydroxybutyrate, you’ll also see Chromium and Vanadium. And guess what?? I did hair testing (the hair toxic and essential elements kit) last year and BOTH were low. So I immediately got on both late last year and figure I’ll need to stay on those the rest of my life. I also take the recommended manganese and magnesium. I also use Berberine if I’m going to eat carbs (when I remember). You might say that Berberine is a natural version of Metformin. I comment more on all this in the September 2016 UPDATE below this.
MY FATTY ACID METABOLIC BLOCK
This turned out to be another problem I have towards energy production! It was manifested by my “very high” Suberate and “high” Ethylmalonate, and the recommendation is a strong need for l-carnitine and B2.
Suberate is another organic acid and is the product of your fatty acid metabolism. Like glucose, fatty acids are an important source of energy! They are formed from carbohydrates in your diet then processed in your liver, and it involves many important steps, aka fatty acid metabolism. With me having two of those organic acids very high, OAT explains they are strong markers for deficiency of carnitine.
From http://www.functionalmedicine.net/pdf/Insider’s%20Guide_37.pdf:
Carnitine is needed to move fatty acids into the mitochondria where they are converted to energy using vitamin B2. When insufficient levels of carnitine or vitamin B2 slow down this process, other parts of the cellular machinery take over and make adipate and suberate. A similar block in another pathway causes high ethylmalonate. Since most of your body’s energy is produced from the burning of fatty acids, your muscles and brain suffer when this cellular energy pathway is blocked. Anything that interferes with the normal fatty acid oxidation may reveal high levels of these metabolites. Rule out environmental toxin exposure, excessive aspirin use
So because of this issue in my fatty acid metabolism, I got on L-Carnitine (the Fumarate version) many months ago at 2400 mg. There are other varieties of Carnitine, like tartrate, but research told me that the fumarate version is better for ATP energy, and supposedly is absorbed better than tartrate or pure carnitine. Don’t know if it’s accurate but went with it anyway. I also got on high dose B-vitamins since so many recommendations above involve insufficiency of several B’s. I am considering adding extra B2.
But I have to say this: being on 2400 mg l-carnitine and higher dose B-vitamins for a few months has not improved my energy levels at all that I can tell. When something is demanding of my energy, I still have energy/fatigue problems. In fact, as I’m writing this, I majorly crashed when we did a heavy amount of walking over several hours a week ago. That is what spurred me to dig deeper in all this, and implied I need to look deeper into the OAT information I did last year, and increase some other supplements as an experiment, or add additional ones, which I have done with CoQ10, plus adding other supps mentioned above. (Turns out I needed far more CoQ10 and just didn’t know it)
Granted, I do think that my six months of stressful copper detoxing, followed by having to correct Small Intestinal Bacterial Overgrowth late last year (which seems to be caused by my high copper and detox) could have stressed my body and made my Citric Acid/Krebs cycle problem worse…thus, I’m not ready to do as much as I want without crashing like that.
MY HIGH LEVELS OF LACTIC ACID
To my horror, I found out I had high levels of L-Lactate (which can be due to insufficiency of CoQ10) and very high levels of D-Lactate (which could be from the high levels of intestinal bacteria I had last year). More on the latter farther down. But I am really NOT surprised. Looking back, I’ve always been a “lactic acid babe”. I just thought it was due solely to my Mitral Valve Prolapse. I then noticed that if I got low iron (which can be common when poorly treated for one’s hypothyroidism), up went my lactic acid as evidenced by the burning in my legs when I walked up stairs.
This page http://nutritionreview.org/2013/04/krebs-cycle-intermediates/ states:
When oxygen is unavailable or the Krebs’ cycle is inhibited, the body shifts its energy production from the Krebs’ cycle to the Embden Meyerhof pathway of glycolysis, a very inefficient way of making energy.
As well as producing far less energy, glycolysis also produces lactic acid as a byproduct. Increased lactic acid is a common acidotic condition that can be caused by a variety of metabolic problems.
i.e. when I am demanding more energy from my body than usual, and because I have a defective Krebs cycle, my body is producing more lactic acid as an alternative source for energy to meet the increased demand!! But more lactic acid causes more fatigue! When I overdid my activity last week by bounds, I could tell my lactic acid went WAY up with my horrible fatigue. I get these feeling of “inflammation” all over my body, for lack of a better word. It’s horrible.
Concerning lactic acid, http://www.functionalmedicine.net/pdf/Insider’s%20Guide_37.pdf states:
Lactate is the principal product of glucose metabolism in skeletal muscle and is a major player in anaerobic energy production and gluconeogenesis. High levels are commonly associated with coenzyme Q10, biotin and lipoic acid deficiencies. The following should be ruled in or out to determine the underlying reason why lactic acid is elevated: overwhelming infection, hypoxia, high intake of acetaminophen, increased consumption of alcohol, cocaine, increased iron levels, drug side effects (metformin). Rule out diabetes. High lactate can cause muscle cramping, fatigue and brain fog. If HIGH Consider supplementing with CoQ10, Vitamin B1, B2, B3, B5, Lipoic acid and Biotin.
i.e. what it says to rule out doesn’t fit me…except the mention of diabetes. I don’t have diabetes, but I DO have an inherited carbohydrate metabolism disorder which has similar problems! The latter may be pushing my l-lactate up! But so could my tendency to have CoQ10 deficiency!! This study shows that CoQ10 lowered lactic acid in 24 hours: https://www.ncbi.nlm.nih.gov/pubmed/10358830 Another reason why it seems critical for me to be on CoQ10, plus higher amounts, I believe”
The above did make me wonder if somehow, I’m not getting enough oxygen and thus creating more lactic acid, as well. I need to understand this better.
There is much more to say about high levels of lactic acid, but the bottom line…it’s NOT good and has many consequences. One thing I’m taking to counter it is l-Carnosine 1000 mg (not “carnoTine”, but carnoSine). It’s known to buffer lactic acid! This article explains it’s lactic acid buffering quality: http://www.wellnessresources.com/health/articles/carnosine_amazing_benefits_for_athletes_heart_brain_eyes_and_diabetes/ And here’s a great article about it that doesn’t even mention how it will buffer lactic acid, but so many other benefits! http://www.lifeextension.com/magazine/2011/1/Carnosine-Exceeding-Scientific-Expectations/Page-01
And my fingers are crossed, but after almost a week of taking carnisine, I actually think I notice less “burn” in my legs when climbing stairs. So we’ll see…
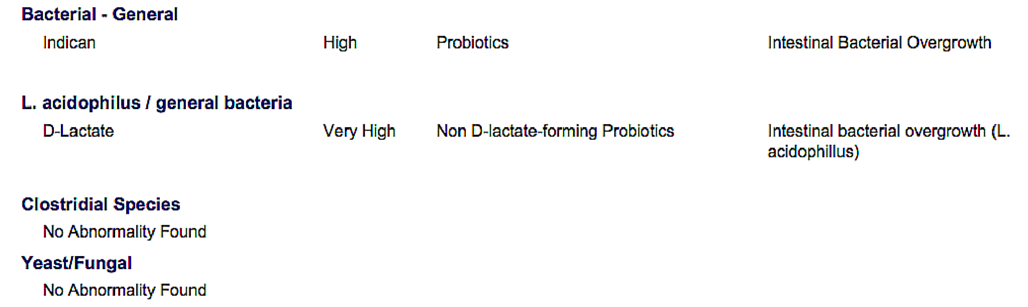
SMALL INTESTINAL BACTERIAL OVERGROWTH (SIBO)
Boy was I shocked to see I had this. Have never in my life had gut issues…and it could be because of the high copper and detoxing. It was revealed by the high Indican and the very high D-Lactate. Now granted, I did not do a thing about it last year when I first saw these high levels in mid-summer, because I had no symptoms. I was clueless.
But by October, I was starting to have problems. I would eat certain evening meals, then within a hour, BAM—becoming extremely bloated and uncomfortable. That’s the bacteria giving off gas in the upper intestines and moving into my stomach. Or, if I ate too much fiber, BAM–I’d wake up in the middle of the night with pains. That’s when I relooked at my OAT and saw that I had too much Lactobacillus acidophilus, aka L. acidophilus!! That’s what is in yogurt! And I’ve always been an avid yogurt eater.
Turns out that Lactobacillus acidophilus is a D-lactate-forming species of bacteria, which explained my high levels of D-lactate. Who would have guessed. But it’s not the first time that I’ve overdone my love for a certain food, in this case yogurt. I’ve done the same with my love of chocolate—I’ve overeaten it so much that I found myself with high levels of oxalates and massive hives as a result. Then a few years later, my overeating of chocolate on top of high stress (which depletes zinc) pushed my copper levels up!! Argh.
I was then faced with dealing with the bacterial overgrowth last Fall. I did a lot of research and chose natural antibiotics to lower my entire bacterial count. I had some Keflex on hand, though, and did nine days of that (even though I’m not sure it helps lower bacteria in the small intestine). Then did Oregano Oil and Berberine for about ten days, then garlic caps (pure allicin) and ginger. And voila…I did it SO well that a yeast infection from hell took over, which NOTHING touched. I still have touches of it after 2 months, but it’s much better.
I’m now on a probiotic called Align, which has the important bacteria Bifidobacterium infantis in it and which SIBO experts say is important. I will move to a different one after having been on Align for three months–probably Culterella based on recommendations in repopulating my gut with good bacteria and to crowd out any remaining bad bacteria. I do NOT want to go through THAT misery again. No.
I used this website a lot by Dr. Allison Siebecker: http://www.siboinfo.com/ but there are many other good ones! So search. Learn.
MY SUPPLEMENTS as of Feb. 2016
Putting this together took a lot of work, and as you see, I haven’t yet figured out all the amounts as precisely as others.
- L-Carnitine Fumerate 2400 a day (same as the last few months) – for fatty acid metabolism problem
- CoQ10 500 mg a day (higher then before) – for energy metabolism; OAT shows insufficiency!!
- Riboflavin (B2) and B3 – needed for ATP. I like ATP Cofactors by Pure Essence–has 100mg of Riboflavin and 500mg of Niacin–but that much niacin caused me to feel quite cold, so am lowering it. Also on a multi-B vitamin and have bought a simple B2 capsule.
- Molybdenum (same) – needed for mitochrondrial, helps lower sulphur, was low on hair tissue
- Manganese (same) – helps lower sulphur (mine is quite high)
- Chromium and Vanadium (same) – for my carbohydrate metabolism disorder, both low in hair testing
- Enzymes– to help me break down proteins since I don’t do that well
- Magnesium 400 mcg – helps ATP and improves energy, fires up enzyme reactions
- Amino Acids (using up the Now brand of Amino Complete) – supports Krebs Cycle/energy. Needed with my Mito insufficiencies.
- Arginine 500/ Ornithine 250 – to lower high sulphur, aluminum, and OAT shows insufficiency of arginine
- L-carnosine 500 mg (new, twice a day) – to counter lactic acid, which body makes with my inefficient energy metab. I am taking two and boy does it work.
- Kreb’s Cycle Intermediates by Enzmatic Therapy – Not impressed. The intermediates were taken out, so just taking it for the magnesium amount. Other minerals are paltry. Using up the bottles and will get no more
- D-Ribose (new) 10,000 mg – this is a sugar used to restore ATP, BUT it can raise my bacteria over time (SIBO), as one guy found out and reported on a website. SO I will only use it when needed.
- Creatine – stimulates the production of ATP–one scoop
- AAKG Arginine Alpha-Ketoglutarate – the latter is a Krebs cycle intermediate I wanted to try, one of the few that aren’t high–1 tsp, plus more arginine. But eventually discontinued this.
- UPDATE: I have added NT Factor, twice a day. Studies show excellent energy improvements on this since it supposedly improves the lipid membrane of a damage mito. Also see https://www.youtube.com/watch?v=5Llvh4bQ7hk
Note: there is often mention of using ALA (Alpha Lipoic Acid) since it is an essential co-factor in energy metabolism, is an anti-oxidant,and improves carbohydrate metabolism. But there is information that it could raise mercury, and I have plenty of fillings. My hair test did not show high mercury, so unsure what to think. May not use it.
SUMMARY
All this is potentially huge. The more I’ve learned, the more I’ve had many ah-ha moments when I looked back at my adulthood. Sure, getting on natural desiccated thyroid made huge improvements in my life and was like a miracle. But I could still tell some pesky lingering issues here or there–nothing debilitating in the least as it was when I was still on the lousy Synthroid, but pesky here or there. And today, what was pesky feels MUCH worse after the stress of six months of detoxing the high copper, followed by the SIBO and treatment, then the yeast infection. I just know that I’m not liking this at all, and perhaps my OAT can help me turn things around. We’ll see.
And yes, I haven’t mentioned everything up there, but because of the length of this article, I simply decided to stop there. I also have high sulphates, for example.
Here’s an Organic Acids Test that can be ordered and done on your own, then sent back to get results.
********************************
UPDATE WITH A NEW OAT TEST plus more: end of September, 2016
After I wrote the above first section, I was feeling better in 2016, slowly but surely, and doing so much more as the months went by. But I learned the hard way that something was still quite wrong.
A second major energy crash
On Sunday, May 22nd, 2016, I had quite an active day and plenty of energy to do so. Yet, that evening, I crashed in a major way just like I did the past February…horrific debilitating fatigue. I woke up the next day with the same debilitating fatigue, which ended up lasting for weeks. So two days later, I did another lab’s version of an OAT test I had on hand by Great Plains to get a clue, because I thought I was doing everything right, and this made NO sense.
Important note about terminology between the two OATS I have now used
My first OAT was by Organix. My second one is by Great Plains. The terminology of the Great Plains OAT is a bit different. Where Organix would say Succinate, Great Plains would call it Succinic. Or where Organix would say ß-Hydroxybutyrate, Great Plains had 3-Hydroxybutyric. But what was good to see with Great Plains is that it also tested several B-vitamins and more. Of course, the problem is that you can never know if the level they show is “optimal”! But it was interesting. From now on in most cases, you will see my comments like this: Succinate/Succinc. The first is Organix; the second is Great Plains.
What the Great Plains OAT revealed as far as the MITOCHONDRIA (done on May 24, 2016)
Bottom line, my mito seems worse. My Succinic/Succinate was SO high in the range they use that you couldn’t go any higher on their scale. And what does high succinic/succinate point to again?? CoQ10! My first supposition was that 500 mg I had been on was clearly not working. I needed to go higher. My Malic/Malate was still high My Fumeric/Fumerate was slightly over range high, though with Great Plains, whereas it was undetectable a year ago with Organix. Again, almost high was 2-Oxyoglutaric/ Hydroxymethylglutarate.
And again, but on Great Plains, there were clear problems related to eating proteins. My 3-Hydroxyglutaric was high just as it was on Organix as Hydroxymethylglutarate, which is a recessive disorder (inherited) caused by a deficiency of glutaryl-CoA dehydrogenase (GCDH). And voila, this affects your mitochondria. And the recommendations were to lower the consumption of proteins (groan) plus treat with L-Carnitine. Since I’ve been on l-carnitine for almost a year, my supposition is that I need to be higher at 2000 mg again (I used to be on 2400, but lowered).
What the Great Plains OAT revealed as far as YEAST AND BACTERIA
It showed high Arabinose, which is probably due to the horrific yeast infection which I acquired at the end of last year after lowering intestinal bacteria due to SIBO in late 2015 (and the SIBO was due to the Copper detox). Yeast produce arabinose in your intestines, which is absorbed and binds to proteins. Arabinose will tend to block B6, Biotin and lipoic acid says a study I found (didn’t save the link–sorry), and another article says OmegaZyme ULTRA by Garden of Life will eat up the Arabinose, so I’m getting on that. Am already on B-vitamins and Lipoic Acid.
What the Great Plains OAT revealed as far as Neurotransmitter Metabolites
My HVA/VMA RATIO was HIGH, i.e. my Homovanillic (HVA) was above range, and my vanillylmandelic acid (VMA) was lower in its range), which means decreased conversion of dopamine to norepinephrine, and the enzyme responsible for that conversion is copper (mine was too high) and Vitamin C (the latter was VERY low since copper is an antagonist–more later!) This seems to be related to my copper levels all over again. I also had a very high HPHPA, which literature states can cause this high HVA/VAM ratio. (I am hesitant to include links as you will see serious diseases associated with these issues, which I do not have. So if you research this, keep that in mind–they will mention a wide ranges of problems associated with these, starting with the worse, and you may not have the worse, as I don’t). The bottom line of all the above is that I need to hugely improve my gut bacteria(5), which I have been working on, and still need more work.
My Quinolinic/5-HIAA (serotonin) Ratio high, which means neural excitotoxicity in brain, but is also associated with excessive inflammation. Quinolinic acid derived from tryptophan and is an important intermediate that the body uses to make the essential nutritional cofactor NAD (B3). The recommendation is to take l-carnitine and turmeric, as well as NAD, which I am now on in the reduced form. (Update: turns out this high ratio/brain inflammation was caused by lingering mold in me, which I didn’t know when I originally wrote this section. I will talk about this in the third red update below for early 2017.)
What the Great Plains OAT revealed as far as KETONE & FATTY ACID
I still show high 3-Hydroxybutyric/ß-Hydroxybutyrate, which information says indicates increased metabolic utilization of fatty acids and l-carnitine recommended, and which Organix had said was a Carbohydrate Metabolism disorder.
But this time I researched more, especially on the “Impaired Isoleucine Metabolism” that Organix had revealed due to a very high B-Hydroxyisovalaterate amino acid…and I found that the latter pushes up the 3-Hydroxybutyric/ß-Hydroxybutyrate!! And the treatment?? Biotin and B2. In fact, the Wiki article on an Isoleucine(6) says this: “Biotin, sometimes referred to as Vitamin B7 or Vitamin H, is an absolute requirement for the full catabolism of isoleucine (as well as leucine). Without adequate biotin, the human body will be unable to fully break down isoleucine and leucine molecules.” So I have gotten on a much higher dose of biotin. And for awhile, once again, I need to cut down proteins, which is where Isoleucine is housed!!
I also have high ETHYLMALONIC (just above range): Again, fatty acid oxidation disorder (which I appear to have) and carnitine deficiency. Supplement with acetyl l-carnitine again—which if you have paid attention, is recommended to me quite often under several issues I have!
I also have top of the range phenylpyruvic (PKU) due to mutations in the PAH gene which results in low levels of the enzyme phenylalanine hydroxylase. Caused by deficient activity of the enzyme needed to convert the essential amino acid (AA) phenylalanine (phe) to tyrosine. Treatment is with a diet lower in foods that contain phenylalanine and special supplements. Foods to avoid: egg whites, shrimp, chicken breast, spirulina, watercress, fish, nuts, tuna, peanuts/legumes, and lowfat cottage cheese. It says I need PUFAs, aka n-3 and n-6 LC-PUFAs, but will need help on that with my doctor.
MY GENETICS PROVIDED ANOTHER IMPORTANT CLUE to my fatigue
After studying all the above, and especially having continued mitochondrial fatigue issues, I went to my genetics and discovered another piece to this current fatigue issue I’m having: those three homozygous NDUFS7 mutations affecting my CoQ10.
These NDUFS7 genes, when working correctly, convert B3 (nicotinamide) to NAD (Nicotinamide adenine dinucleotide hydrogen) to NAD+ to NADH, the active form. So….B3—> NAD —> NAD+ —> NADH. Its reduced form which is responsible for electron transport in the production of ATP, so when working correctly, promotes good energy in your mitochondria. Also, CoQ10 needs NADH in order for CoQ10 to be transformed into its reduced useable form…i.e. coq10 which is also known as “ubiquinone“, converts to the active/useable form of CoQ10, called “ubiquinol“. So without NADH, it can’t do that.
When not working correctly (which could be happening due to my three NDSFU7 mutations, which may have activated due to the stress of my high copper)….less than optimal energy, since NADH works with CoQ10 and your mitochondria, the energy producing part of your biology.
A lot of literature states that neither B3 nor NAD+ are as energizing as NADH when it comes to supplementation, even though you will find the opposite stated, as well…that NADH is more energizing as the reduced form. Life Extension feels their Nicotinamide Riboside (the latter a precursor to NAD+) is a great product and that “NADH is not effective as a supplement because it is poorly absorbed, due to disintegration in the digestive tract” (said to me in an email). They base that on this: http://www.ncbi.nlm.nih.gov/pubmed/16802695 YET….you will see many reviews of people who see definite results from straight NADH, the reduced form, which is the opposite of what Life Extension is saying. And for someone like me who may not adequately convert NAD to NAD+ to NADH, I may need straight NADH. Right now it’s a supposition, but I’m taking no chances and using straight NADH.
As far as straight NADH, there are some forums which say that no more than 5 mg is necessary, and some are over-stimulated on 10 mg. Then there are people I know who have done fantastic on 50 mg NADH. And guess what–that is now me.
I found that the information by George Birkmayer, M.D., Ph.D.(7) was absolutely the best on NADH. There are videos of his information on YouTube.(9)
Here’s a study showing the efficacy of NADH for chronic fatigue: https://www.ncbi.nlm.nih.gov/pubmed/10071523 And here’s a great article which contains good NAD/NADH info: https://holisticprimarycare.net/topics/topics-h-n/healthy-aging/1607-is-neuro-regeneration-a-reality.html You’ll see that the fabulous Andrew Heyman, MD, who contributed to the STTM II book, is mentioned.
I found that NADH does the following as well (from a book on the net, which again, I neglected to copy the URL when researching–sorry): repairs cell damage, stimulates the immune system, stimulates the breakdown/use of neurotransmitters (which positive affects mood), stimulates the production of Nitric Oxide (NO) which relaxes blood vessels in your heart, lungs, brain and kidney. And….NADH has some very interesting positive results in animals against Alzheimers!(8) Finally, as of 2006, it was stated to be the only supplement with a “scientifically prove anti-aging effect”.
CURRENT BOTTOM LINE:
I moved up to 1500 mg liquid CoQ10 (Liq-Nol, but later moved to Cyto-Q) while detoxing high copper for the second time and noticed much better results!! Studies showed some people have gone as high as 3200 mg without side effects, so that made me feel better. The Liq-Nol is sweetened with sucralose, sadly, so I am experimenting with only 500 mg of the liquid along with Life Extension’s gelcaps Ubiquinol with Shilajit (the latter has research showing it improves CoQ10 uptake). WARNING: I went QUITE downhill when doing all the latter with Health Thru Nutritions 300 mg Ubiquinol from Kaneka QH and do NOT recommend it. I have now added NADH to it (the active form of B3), as CoQ10 works better with it.
My current supplements are as following:
- Acetyl L-Carnitine (and still using up my Fumerate) and making sure it’s at least 2000 mg daily again – for fatty acid/carbohydrate metabolism problem, plus more
- Liquid CoQ10 1500 mg a day (higher then before) – for energy metabolism; OAT clearly shows insufficiency on 500 mg!!
- NADH – 50 mg
- A multi B-vitamin- needed for ATP. I’m currently on Vitamin Code Raw B-Complex, and adding NADH, folate (I also have a folate mutation that I failed to mention above) and more biotin to it, as I clearly need the latter for an impaired isoleucine metabolism disorder.
- Molybdenum, Manganese – needed for mitochrondrial, helps lower sulphur, was low on hair tissue, and I get it from this: Trace Minerals Complex II
- Chromium and Vanadium for my carbohydrate metabolism disorder, both low in hair testing
- Enzymes– to help me break down proteins since I don’t do that well
- Magnesium 400 mcg – helps ATP and improves energy, fires up enzyme reactions
- Amino Acids – supports Krebs Cycle/energy. Needed with my Mito insufficiencies.
- Arginine 500/ Ornithine 250 – had high cis-aconitate in 2015 which is related to Renal ammonia clearance and your energy production, and was now low on the 2016 Great Plains, possibly due to my arginine supplementation. 🙂 But staying on it for multiple benefits.
- L-carnosine 1500 mg (up from earlier this year) – Note that this is carnoSine, not CarnoTine. This not only counters lactic acid, which I can tell I’m still making too much due to mito issues, but is a great anti-oxidant.
- R-alpha-lipic acid said to be a powerful activator of mitochondrial energy and works with acetyl-l-carnitine
- Vitamin D – mine goes too low if I don’t, plus it’s said to enhance mito function
- Culturelle (30 million to counter former high HPHPA bacteria and Saccharomyces Boulardii (2-6 billion) to counter same.
- NT Factor I am experimenting with this again. I was taking it in May, went quite high, and it started me detoxing my copper again! Had to get off due to detox fatigue, which I eventually improved greatly with the 1500 mg CoQ10. Using it due to lots of literature stating it help heal damaged mito: https://www.youtube.com/watch?v=5Llvh4bQ7hk
And I am involving my two doctors in all this for more feedback to get out of this chronic fatigue mito problem. 🙂
And by the way, I’m still detoxing high copper for the second time, so I’m supporting my liver and kidneys, plus on antioxidants Astaxanthin and Vit. E, as well.
UPDATE for 2017–I have mold in me! Could this be fundamental underlying cause that lead to all this cascading mess? I think so.
Made an interesting discovery late last year: I’ve still got mold in me from a massive exposure in 2013, even though I had treated it then and felt better. It has apparently wrecked havoc in me all this time, and which can partially explain my mito issues. The mold damaged my mito somehow! And the high copper made it even worse.
Why do I still have that mold in me?? Testing (HLA DRB, DQB Panel) revealed that I am part of 24% of the population who have genes that make us more susceptible to getting very sick from the super tiny “biotoxins”, plus makes it more difficult to get the mold out of me…even though I thought I had. I also did the C4a test–double the top of the range and classic for mold inflammation. C3a was fine. Other tests were done to confirm all this. I am in treatment now to get this mold out of me.
In March 2017, I did a Spectracell nutrient test while I was experimenting with 1000 mg liquid ubiquinol and felt well on it…yet Spectracell showed that was the ONLY thing I was “functionally deficient” in i.e. CoQ10. Shocked me. I had to go back up to 1500 mg liquid ubiquinol, which is a financial killer. And I’ve learned the hard way that on days of high activity, I’ll probably require more.
In May of 2017, I thought more deeply about something else: CoQ10 is made from two amino acids: L-Phenylalanine and l-tyrosine. And since my OAT test revealed that I don’t break down protein correctly, that can mean that I don’t have enough l-tyrosine (which L-Phenylalanine breaks down to). I am experimenting with l-tyrosine supplementation soon to see what happens–can’t take L-Phenylalanine as it’s not recommending for PKU, which I don’t break down correctly either.
Footnotes:
5. http://integrativemedicineformentalhealth.com/articles/shaw_hphpa.html
6. https://en.wikipedia.org/wiki/Isoleucine
7. http://www.nadh-priceinfo.com/nadh_doctor_birkmayer_interview.cfm
8. http://nadh.com/pages/alzheimers
9. https://www.youtube.com/watch?v=lm6-C78Zank
Important notes: All the information on this website is copyrighted. STTM is an information-only site based on what many patients worldwide have reported in their treatment and wisdom over the years. This is not to be taken as personal medical advice, nor to replace a relationship with your doctor. By reading this information-only website, you take full responsibility for what you choose to do with the information on STTM or its outcomes. See the Disclaimer and Terms of Use.