In Loving Memory of Dr. William Trumbower, a Contributor to the STTM II book
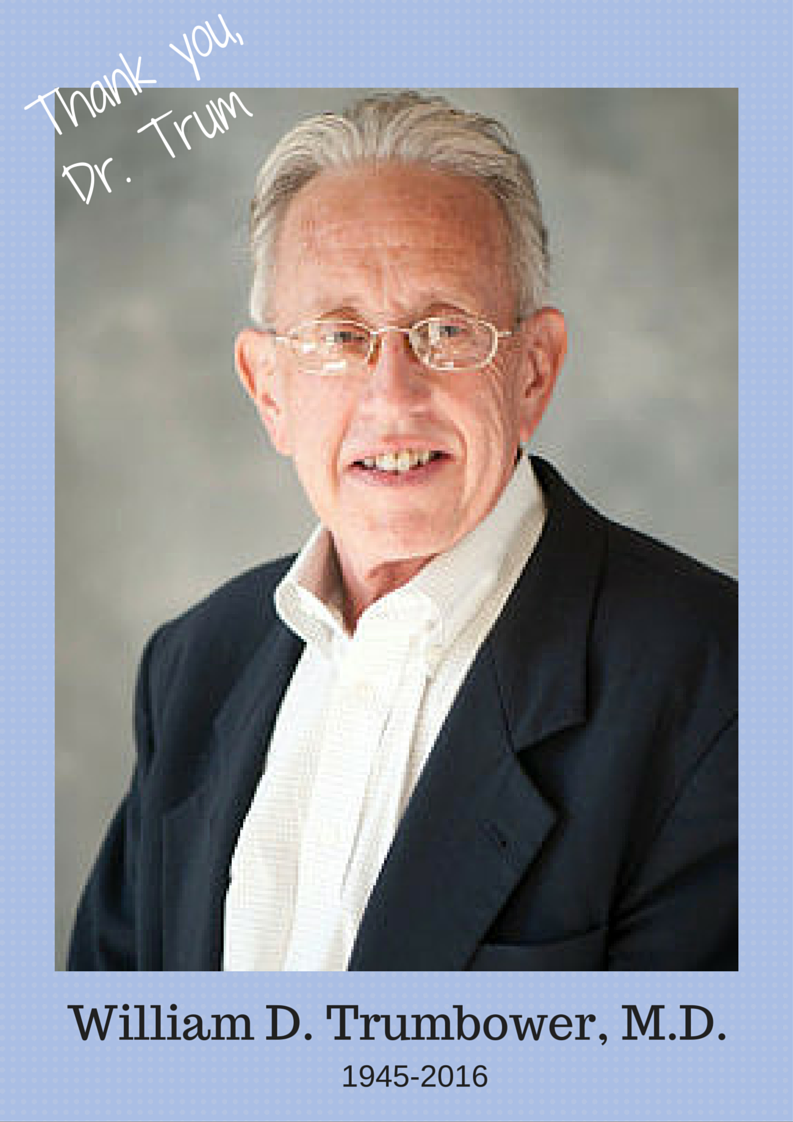 With great sorrow, I want to announce that Dr. William D. Trumbower of Missouri, who contributed the chapter Nutrition and Hypothyroidism in the Stop the Thyroid Madness II book, has recently passed away.
With great sorrow, I want to announce that Dr. William D. Trumbower of Missouri, who contributed the chapter Nutrition and Hypothyroidism in the Stop the Thyroid Madness II book, has recently passed away.
I adored Dr. Trumbower. He had great humility. When I asked him to be in the book, he stated that he “agonized over it as I am not in the same category as the other authors”. Posh!! I knew that was totally wrong. He was smart, open-minded, insightful and fabulous.
What I loved about his chapter is his take on the effects of either inflammation, malnutrition or toxicity on one’s hypothyroid state. He talked about the gut and the problem one can have from gluten, besides all the problems we can encounter from refined sugars and industrial-processes oils–all which he explained can cause more inflammation.
In one section of his chapter, he discussed the problems on our thyroid and health in general due to toxicity from halogens, heavy metals and xenoestrogens. I kept thinking about that when I discovered myself with high copper and lead last year, as well as high barium!! He was also keenly aware of the importance of knowing if one has the MTHFR mutation, which in itself can cause high heavy metals.
Dr. Trumbower believed that “almost all hypothyroidism begins as a nutritional disorder”. Patients haven’t always found that to be true for them if genetics are involved, but we agree that a high body of us could fall in that nutritional problem category!! So what a perfect chapter subject for him to focus on.
But here’s what I have NEVER forgotten about Trumbower: He followed his own advice about nutrition and stated that his “thyroid dose dropped from 150 mg of desiccated thyroid to 30 mg daily”. That has always blown me away. His experience underscored how important it is for all of us to know our nutritional status and treat it! I definitely do. I had found myself to be low in B-vitamins, l-carnitine and CoQ10 and definitely treat those. I also tend to fall too low in magnesium, so that’s an important nutrient for me to supplement. Dr. Trum certainly underscored it.
After the STTM II book came out, he explained to me in his own humorous way how it had changed his professional life. He stated: “I now have credibility instead of being an old outlying radical doc.” Don’t you love it?? Now you know why I found him to be so endearing. And one way he blessed me in return is in stating that even he used the revised STTM book to guide his own thyroid journey! You make this girl proud.
In 2015, Dr. Trumbower and his daughter Elisabeth created a fully integrated clinic that combined aesthetics, wellness and bioidentical hormone therapies, called Pela Cura Anti-Aging & Wellness. What a blessing that must have been to worked with his own beloved daughter!
I have included his bio from the book below, just for you to know more about him and what a wonderful person and doctor he was!
Rest in Peace, Dr. Trumbower. Your chapter in the STTM II book will forever inspire thyroid patients, just as your presence and open-mindedness in the lives of so many of your patients have done the same.
********************
I, William D. Trumbower MD, am a 69-year-old OB/GYN (no longer doing obstetrics or surgery), practicing in the, medium size, college town of Columbia, Missouri. I am blessed in my practice, as my eleven partners do not require me to take call any more. I am able to spend my time, in my office, performing annual exams on many people I have known for well over 30 years, as well as being able to concentrate on bioidentical hormones, thyroid, chronic fatigue and other areas that no one seems to be very interested in, probably because they are not extremely profitable.
I did not mean to be an alternative thyroid hormone physician. Nothing in my training would have given me any hint that this was to be my destiny. During my residency, I was obsessed with surgery, high-risk obstetrics and obstetrical anesthesia. I was fortunate enough to to stay on the teaching faculty, at the University of Missouri — Columbia, for three years, as an assistant professor. I left the University of Missouri and entered private practice, in 1979.
I suppose I can trace much of my interest in alternative thinking to my parents, who were both extremely bright and well-read individuals. My father, who had been a captain, in World War I, was the product of a classic East coast education and seemed to know everything about everything. My mother was a registered nurse and she was the one who directed me into medicine, by forcing me to get a job, in the summer of my high school graduation, in 1963, as an orderly, at the University of Missouri Teaching Hospital, in Columbia, Missouri. When I think back to my youth, one of the turning points, at the age of 15, was reading Immanuel Velikovsky’s book’s Worlds in Collision and Earth in Upheaval. I realized, after reading these books the important issue for me was not whether Dr. Velikovsky was right or wrong about his theories (I believe he was right, about most things), but how the scientific establishment dealt with someone who dared to question consensus views. This attitude of not accepting what everyone assumes is the truth has stuck with me for the rest of my life.
Another turning point, for me, and my career, occurred early in my private practice, in the 1980s, when I was confronted with patients with cyclic mood problems, which my training had not prepared me to deal with, at all. The only thing that I could think of, for people like this, was hysterectomy and putting them on Premarin. One of my patients directed me to the works of Dr. Katharina Dalton, in London, England. When I tried some of her techniques of supplemental natural progesterone, I was astonished to find that it worked remarkably well. As a result, my family and I took a trip to London, where I spent a week with Dr. Dalton learning her techniques. When I returned home, full of enthusiasm to share my new knowledge, I was shocked to find that most of my colleagues were very negative and wanted nothing to do with this information. It literally drew a line in the sand, with me on one side and most of my colleagues on the other. However, when I looked around, most of the patients were on my side of the line.
Because of my age, I did some of my training in the days before Synthroid dominated the market and natural products, such as Armour, were still in wide use. My mother was hypothyroid and I watched as her new doctors switched her to modern medicines, leaving her with a continued weight problem and fatigue. Because of this, I was open-minded enough to prescribe Armour, if patients requested it, but I really did not know much about it until I met another physician from Columbia, Missouri, Dr. Mark Starr. Mark was from Columbia and moved back here to start a practice. He is the author of the book Hypothyroidism Type 2. I realized that he had a lot to offer my patients and so I began to communicate with him. He is the one who directed me toward the work of Dr. Broda Barnes and opened my mind about thyroid. Since then, I have continued to read and study, extensively, about thyroid. My education was enhanced when I was diagnosed with Hashimoto’s thyroiditis, in the last decade.
Interestingly enough, one of my patients had brought me one of the first editions of Stop the Thyroid Madness, prior to my diagnosis. I actually used many of the techniques and suggestions, in the book, to guide me through my own hypothyroid treatments, including a trial of Synthroid, finding elevated reverse T3, having to use T3 only and, finally, settling on desiccated thyroid, which I have been on since that time.
When Janie Bowthorpe called me to ask me to write a chapter, for her new book, I was dumbfounded to find that anyone knew who I was. I was likewise astonished at the other authors in the new book, many of whom are people whose works I regularly read. My hope is that this chapter will provide a small overview of my view on thyroid disease and the general approaches that I take with it. I will end by saying that the most powerful tool that anyone has to control their health destiny is what they eat every day
** Dr. Trumbower’s obituary http://www.columbiatribune.com/obituaries/bill-trumbower/article_60ba8e47-c38f-5f03-ad9a-a87978dfa9ef.html