Feel better on T4 than you did on Natural Desiccated Thyroid?

Occasionally, hypothyroid patients will exclaim with conviction and truth that they outright feel better on Synthroid or Levothyroxine (T4-only meds) than they did when they tried Natural Desiccated Thyroid (NDT) or even T3-only. And we believe them.
But…there is an explainable reason which does not mean T4-only is better for you. It really isn’t. Bear with me and read on…
Years ago, as many of us were starting on NDT after being on T4, we were seeing our lives change in a huge way, far more than T4 did! It was like a miracle! Those five hormones really made a difference.
But some others were having problems when raising something so miraculous for others. Huh?? We didn’t get that.
It took awhile longer to finally see why and to answer the “huh?” i.e. we began to see that there were three strong and correctible reasons why someone was not seeing the miracle of NDT as others were, and instead, were blaming the NDT (or T3) and moving back to T4-only…
The three main and correctible reasons why NDT, which gives all five thyroid hormones, seems to fail…
1) NOT BEING “OPTIMAL” WITH YOUR NDT DOSE (it’s NOT about just being in range and not about being held hostage to the TSH)
We all have had a tendency to believe that our doctors know what they are doing with NDT or T3. But, the majority do not. They tend to leave you on too-low doses, and/or pay attention to the lousy TSH. Thus, due to the natural suppression of the feedback loop (hypothalamus to pituitary to thyroid), you will get worse on those lower doses, sooner or later. i.e. you will get more hypo, and/or have rising adrenaline, cortisol, anxiety or other. And because of that, some exclaim “NDT didn’t work for me!” and they rush back to T4-only. But NDT, with all five thyroid hormones, could have worked well IF you had known to be more optimal. Optimal puts the free T3 towards the top of the range and the free T4 mid-range, and puts the TSH below range…all three…and removes all symptoms. What amount does that is very individual—some start to achieve that in mid-2 grains, others are in the 3-5 grain area, others may be higher.
What if you tried to raise to be optimal, but had worsening problems? Read #2 and #3 below.
2) NOT BEING OPTIMAL WITH YOUR IRON LEVELS (it’s not about just being in range)
When this is brought up to patients who once tried NDT and failed, they will exclaim with all sincerity “But my iron levels were great”. We know that a very small percentage may have had good iron. But what is common with the majority is they did NOT have good levels “Falling in the normal range” does not equal a good level of iron. It’s WHERE one falls that tells the story.
For example, with two types of ranges for serum iron (NOT ferritin):
a) When the range is approx. 40?155: women who have optimal serum iron tend to be close to 110, or 109, or 108, etc. They are NOT in the 90’s and definitely not lower when optimal. Men tend to be in the upper 130’s.
b) When the range is approx. 7-27: women are optimal around 23ish; men are towards the top.
If they are lower than the latter examples, it messes up the ability to raise NDT and feel great without issue. Why? Inadequate iron levels tend to raise the reverse T3 (RT3) as one is raising their NDT. As the RT3 goes up due to inadequate iron, you will feel worse. And because of that, some exclaim “NDT didn’t work for me!” and they rush back to T4-only…but if they had had optimal iron, NDT WOULD have worked…as long as they also had optimal cortisol (See #3 below) and were working to find their optimal dose of NDT (see #1)
See more details about iron here: http://stopthethyroidmadness.com/ferritin
3) NOT BEING OPTIMAL WITH YOUR CORTISOL LEVELS (it’s not about just being in range, and it’s NOT about blood cortisol)
We noted years ago that at least 50% of those with hypothyroidism had a cortisol issue as revealed by saliva, not blood. What does a cortisol issue mean? Either their cortisol was too high (due to the stress of being undiagnosed, poorly treated, or being on T4) or was too low (due to the stress of being undiagnosed, poorly treated, or being on T4), or had both high and low (due to the stress of being undiagnosed, poorly treated, or being on T4).
And what happens with a cortisol issue when you are trying to work with NDT? Either RT3 will go too high (the inactive hormone), or one’s T3 will pool in the blood and not make it to the cells, or both…and you won’t feel well or have bad reactions like excess adrenaline, anxiety, shakiness, feel-bads.
And because of having a cortisol issue, some exclaim “NDT didn’t work for me!” and they rush back to T4-only…but if they had…
a) done the 4-point saliva test, not blood
b) compared the saliva results it to the lab-values page (it’s not about that normal range)
c) CORRECTLY treated it (see this page, plus Chapter 6 in the updated revision STTM book if saliva is VERY low, which also applies to Adrenal Cortex),
….they would have soared on NDT…along with good iron and being OPTIMAL on NDT (or T3)
Note: it’s always about the results of a saliva test, NOT blood cortisol.
Bottom line, it’s not as simple as “feeling better on T4”. It’s more about that you are NOT experiencing the side effects that you did on NDT from any of the above three problems, which were all correctible. That is different.
“That all sounds like too much trouble–I’m staying on T4-only!”, you may be exclaiming….

There is a big problem with that reasoning that I hope you will be open to….Namely, T4-only outright…
- CAUSES low iron
- CAUSES a cortisol problem
- CAUSES many other issues like lowered B12, lowered Vitamin D, rising blood pressure, rising cholesterol, depression, anxiety, heart issues, bone thinning, chronic pain….and more. The individuality is in who gets which…but T4 users do get problems of their own kind, sooner or later.
Please note that the above is not an empty strong opinion. It’s based on years of reported patient experiences from many who were on T4! i.e. most of the following hypothyroid symptoms were experienced by T4 users!! They were still hypo!
Now you may state “But I know people on T4 who do not have those problems!”.
First, some outright DO have some of those problems, but don’t realize it or they deny it (while others see it in them). Adrenal issues, even those denied, can make certain people awash with defensiveness, argumentativeness, denial, anger, paranoia towards others observations, low patience, moodiness, etc.
Yes, some on T4 do, in fact, do better than others. But you know what we have observed? The longer they stay on T4-only, the more problems WILL, in fact, raise their ugly heads eventually…like either adrenal issues, or low iron, or low B12, or depression, or rising cholesterol, or rising blood pressure, or heart problems, or dry skin and hair, or chronic pain, or bone loss, or rising illnesses…..on and on. Forcing the body to live for conversion alone backfires….sooner or later.
 Summary: A working Natural Desiccated Thyroid, or adding T3 to that T4 as a second choice and getting those frees optimal, is a much better way to go than being on nothing but T4, according to years of worldwide patient experiences
Summary: A working Natural Desiccated Thyroid, or adding T3 to that T4 as a second choice and getting those frees optimal, is a much better way to go than being on nothing but T4, according to years of worldwide patient experiences

A working NDT gives you all five thyroid hormones, and does NOT force you to live for conversion of T4 to T3 alone, i.e. some of NDT is direct T3. Additionally with T4-only, some people have genetic mutations which hinder the conversion of T4 to T3 and may not realize it.
There is a good reason that millions of patients found out that T4-only is not the way to go for many reasons, and NDT is the way to go if you correct the reasons you did NOT to do well...or even adding T3 to your T4 in an OPTIMAL amount. But you will still need optimal iron and cortisol!
P.S. The above three reasons are the most common for not doing well on NDT (or T3) and should be considered first. A 4th less common reason: chronic inflammation of any cause. Read about inflammation. If this is true for you, the sad part is that T4-only will also backfire, as it raises RT3.
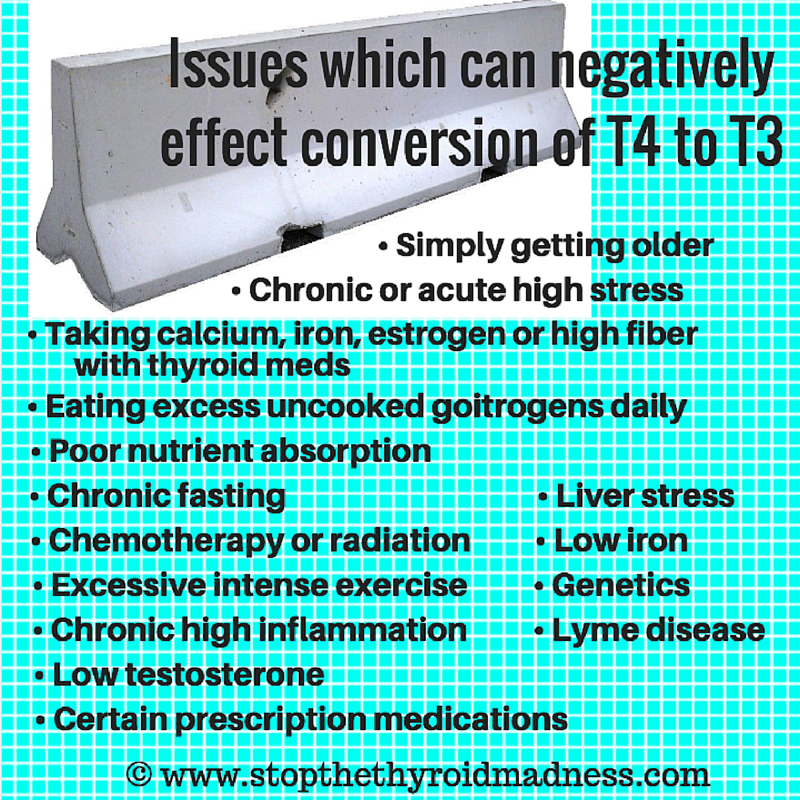
Mold exposure can also effect conversion.

Click on the graphic to order an excellent saliva cortisol test.