How Dawn healed her adrenals–an inspiring story everyone must read!
 When I first had my thyroid removed in 2012 due to autoimmune destruction from Hashimoto’s disease since age 10 and Graves disease for 6 years, I did not know what to expect. And like most other post-thyroidectomy patients, I was reassured by my surgeon that all it would take is for me to take “a little pill every day and things will be much better” (i.e. my surgeon referring to the Synthroid she prescribed for my post-op thyroid replacement)
When I first had my thyroid removed in 2012 due to autoimmune destruction from Hashimoto’s disease since age 10 and Graves disease for 6 years, I did not know what to expect. And like most other post-thyroidectomy patients, I was reassured by my surgeon that all it would take is for me to take “a little pill every day and things will be much better” (i.e. my surgeon referring to the Synthroid she prescribed for my post-op thyroid replacement)
What ensued after that was a nightmare that has lasted the past two years!
I went into heart failure multiple times from the inadequate replacement with Synthroid (T4 only medication). I was MISERABLE! Dizzy, heart racing out of the blue, internal shaking as well as nausea, severe fatigue and extreme irritability! I became a monster that even my own family did not recognize!!
STTM was discovered
Fast forward 9 months, and a good friend of mine came across the Stop the Thyroid Madness website and sent it my way. I ordered the book after looking through the website and realized I knew NOTHING about thyroid disease and proper treatment for hypothyroidism, and apparently neither did my Doctor!!
I made the switch to a working Natural Desiccated Thyroid like Armour e in March 2013, and things DID improve some. But the fatigue, shakes, dizziness and irritability continued! I flew off the handle at my husband, my parents, even my dogs (poor babies did not deserve it, but I was just out of control emotionally!) I thought I must be going crazy and feared I had developed a psychiatric disorder. In fact, my Endocrinologist suggested I see a psychiatrist to “work out my frustration and anger!”
It was my adrenals!
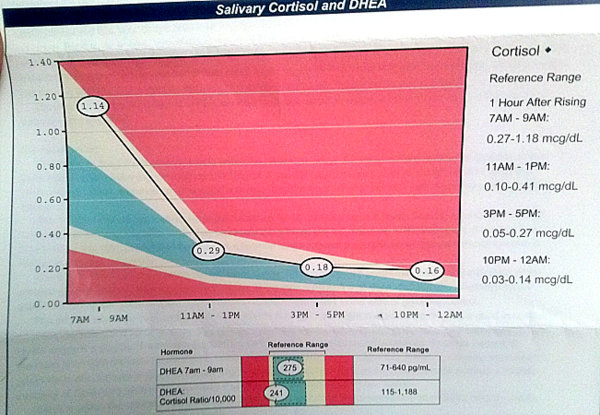
I started reading Chapter 6 in the revised STTM book– All about ADRENALS!! I thought I was reading my life story all over again! I had 90% of the symptoms listed on the “symptoms of low cortisol” page on the STTM site. I tried Janie’s at home testing and failed them all miserably! I ordered a 24 hour adrenal saliva cortisol test, and there is where I found my answer! See the results below:
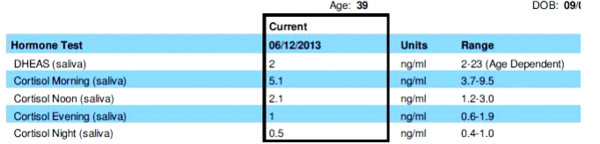
Turns out I wasn’t crazy! My adrenals were not putting out adequate cortisol to handle the increased stress of low thyroid levels and all my other life issues! I was LOW, LOW, LOW, slightly HIGH.
“How do I fix it?”Â
I considered using T3CM, but knowing that I was low Morning, Noon AND Evening meant that was not likely to help per other patient’s experiences.
So someone suggested I try Thorne ACE (Adrenal Cortex Extract) to replace my low cortisol at those three times of day! I got it all ordered, read through the chapters in the STTM book. I added in high doses of Vitamin C (3,000mg per day) and high doses of magnesium (800-1,200mg per day) and started supplementing with Celtic Sea Salt and the Adrenal Cocktail (salt in water, plus minerals). I started feeling better pretty quickly with the sea salt and nutritional support added.
It took me several weeks of trial and error to get my symptoms under control and get the dose of ACE correct. I had to learn to take DATs (Daily Average Temperatures) to gauge whether or not the dose was the right one. I tracked symptoms, doses and temps daily. I adjusted up every few days until my temps stabilized and my symptoms became more minimal. I was still without a good doctor at this point, so I was self-treating using the knowledge I got in the support groups and in the Stop the Thyroid Madness book.
A job change was necessary
I realized that I could not continue under the extreme stress of working the 12 hour nightshift in a busy hospital. I was burning the candle at both ends, and everything I read about adrenals said reducing stress and sleeping on a set schedule was a MUST. So, I spoke with my spouse, and we decided I would quit my job and look for something less physically and emotionally demanding, and something with day-time hours exclusively. I was off work for 3 months while searching for a new position, and though money was tight and things were stressful, changing to sleeping at night once again made a HUGE difference (I put myself on a strict 10 pm-7 am sleep schedule.) I cut caffeine, sugar and alcohol out completely — the caffeine was very tough to give up, but I did it! Being out of the high-stress work environment was extremely helpful in healing adrenals!
A saliva retest
I was feeling better little by little, but the fatigue remained, especially in the afternoons. I would just crash around 2 pm and couldn’t do much of anything until late in the evening! I would get periodic adrenaline reactions (especially late in the afternoons.) I would sweat profusely, get shaky inside, feeling like my heart would pound out of my chest! I finally got in to see my “good thyroid doctor” in November 2013. He immediately said he wanted to take me off ACE for two weeks and retest my adrenals to see if I had made progress. Here is what they showed: (the retest is the one that says “current” taken in November 2013:

As you can see, my Morning was showing improvement, but the noon and evening levels slid to a lower level than when I started ACE.
I spoke with my good thyroid doctor, and he suggested we lower ACE in the morning, add more at the noon/evening doses and slide the times a bit earlier than what I had been taking. Things continued to improve, and I got my afternoons back! By then I was back working full time up to 50 hours per week. The new job was emotionally stressful, but not physically so. I continued to get adrenaline reactions in the late afternoon, but they became less and less as time went on. I started feeling completely recovered by Feb 2014. I still had low thyroid levels due to hormone resistance, but adrenals symptoms had completely resolved. I weaned off ACE and did just fine. I kept up with the nutritional support of high dose Vitamin C and Magnesium and did the adrenal cocktail and celtic sea salt if I needed it, but it was rare for me to need those at this point.
Victory!
We waited three months of me being off of ACE and retested to see where I stand! Here are the new, post-treatment levels. Taken end of April, 2014:
As you can see, my levels are now VERY close to optimal! I did notice that my nighttime level has gone up some, so my doctor had put me on Zinc to help reduce that, and Melatonin as needed (though I don’t really take it more than once per month.)
I discovered recently that I have Lyme disease and chronic infections which is the cause of my inflammation and continued low thyroid levels, despite taking Nature-Throid and Cytomel T3 at high doses. We hope that treatment for Lyme will finally help get inflammation down and improve my thyroid levels to liveable again!
I cannot be more thankful to Stop the Thyroid Madness for helping me get my life back! There IS life after Adrenal Fatigue!! I would say healing my adrenals has been the single most important thing I have done to feel better and function better on a daily basis. My family and my dogs no longer fear me and I have my laidback personality back once again, and my house is now at PEACE!! Don’t give up hope!! STTM will help you get better if you follow it!
*******************
* Are you signed up to receive notifications of these blog posts by email? Scroll down to the bottom right on the STTM home page to sign up: https://www.stopthethyroidmadness.com/
* Are your Ducks in a Row??https://www.stopthethyroidmadness.com/ducks-in-a-row
* Janie Bowthorpe has the first of a series of eBooks out, and the first one is on EBV:https://www.stopthethyroidmadness.com/sttm-ebooks/